See how elevation data reveals the greatest truths about corneo-scleral shape.
By Aaron Wolf, OD
The evolution in corneal and scleral shape assessment has shifted towards the use of sagittal height elevation data rather than traditional curvature measurements. This change is significant for practitioners and manufacturers alike, particularly in the realm of contact lens fitting and anterior segment imaging.
“Corneo-scleral profilometry is particularly valuable in scleral lens fitting for both simple and complex ocular geographies.”
This two-part series explores the tools for understanding cornea and sclera shapes: part one focuses on diagnostics, while part two (coming soon) will cover how to use these technologies to improve lens fitting practices.

Aaron Wolf, OD, FAAO, FSLS, FIAOMC
Here are some key takeaways from the article, highlighting the most relevant insights and discoveries:
Corneo-scleral Profilometry
There are projection-based devices used for ocular surface topography, the corneo-scleral profilometers. The main distinction is that they are designed to derive their principal data from sagittal height elevation differences, not curvature, offering a dramatically better representation of 3D modeling of the eye than prior projection topographers. Corneo-scleral profilometry is particularly valuable in scleral lens fitting for both simple and complex ocular geographies.
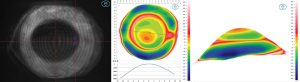
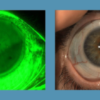
The Eye Surface Profiler (ESP) is able to image over 20mm in a single image capture with over 500,000 data points: projection grid (left), 20mm profilometry elevation map (center) and three-dimensional reconstruction (right) of eye with keratoconus and pinguecula.
Curvature data does not necessarily correlate with sagittal depth (Figure 1). Three similarly shaped corneas with oblate profiles show different ocular shapes and elevation profiles. Patient A has a mean K of 36D and a sagittal height of 3,810µm at 15mm. Patient B has a similar mean K of 42D and a significantly higher mean sagittal height of 4,220µm. Patient C has a similar mean K of 44D but a drastically higher mean sagittal height of 5,130µm. Although their topographical curvature data appears similar, their heights vary by almost 40%. This shows that ocular shape assumptions based on curvature are limited; elevation-based imaging is necessary for accurate assessment. Figure 1 confirms the accuracy of profilometry in representing ocular shape.
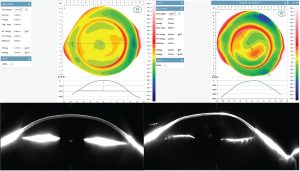
Fig. 1 Notice how precisely the profilometry profile beneath each ESP elevation map correlates to the Scheimpflug tomography slice at the same meridian, confirming the accuracy of profilometry in representing ocular shape.
“Thinking about the cornea in terms of curvature is of little use to describe ocular shape, contrary to prior assumptions. Elevation-based topographical data is the only true way to achieve a full picture for managing the refractive and ocular health of our patients to the best of our ability.”
___________
By Aaron Wolf, OD
Those practitioners who have elevation-based instruments may be at an advantage in gaining a more comprehensive picture of the ocular surface anatomy.